
5 “Diagnoses” to Learn about in October (and year round, of course)
October is a popular month for awareness! We’ve put together a list of 5 diagnoses/topics related to speech, language, and feeding. Keep reading for more info!
ADHD
Attention-Deficit/Hyperactivity Disorder (ADHD) is a mental health disorder that negatively affects a person’s ability to access and use Executive Functioning Skills.
Executive functioning skills help us:
Pay attention
Organize, plan, and prioritize tasks
Start tasks and stay focused until they are complete
Understand different points of view, empathy, putting ourselves in other people’s shoes
Regulating emotions
Self-monitoring (keeping track of what you’re doing within a given task or timeframe)
Source: https://www.understood.org/en/articles/what-is-executive-function
These skills typically develop in early childhood, but children (and adults) certainly can struggle with these areas and not have ADHD. Difficulty with these skills becomes a disorder when daily life is highly impacted. It’s important to remember that ADHD is an actual mental condition. It actually affects how the brain functions. The behaviors seen in people with ADHD aren’t laziness or even a choice.
Here’s an example that may help. Think about how a car gets started. There are several working parts that have to do exactly the right thing at exactly the right time to start the engine. One important part is the starter. People with ADHD don’t have a functioning starter in their brain. They’re ready and willing to go somewhere, but their “car” won’t start. They can develop strategies to improve the functioning of their starter, but they’ll almost always have a starter that is a bit finicky.
Other symptoms that may be less obvious include:
Being habitually late or having difficulty managing time
Difficulty getting started with tasks
Difficulty switching between different tasks
Trouble finding motivation to complete tasks they may actually want to do
Being forgetful
Being disorganized or messy
Needs extra time to process information (may seem like they’re not listening, but then respond once they’ve processed the info)
Daydreaming
Sensitive to noise, textures, emotions
Benefiting significantly from external structure, but have difficulty creating their own structure (i.e. may do well at school, but struggle with getting homework done)
Risky behavior
Hyperfixation (getting highly interested/invested in a particular task, activity, or interest for varying lengths of time)
Treatment can include medication, behavioral modification, specifically addressing executive functioning through therapy, and trial and error with strategies to better access those executive functioning skills.
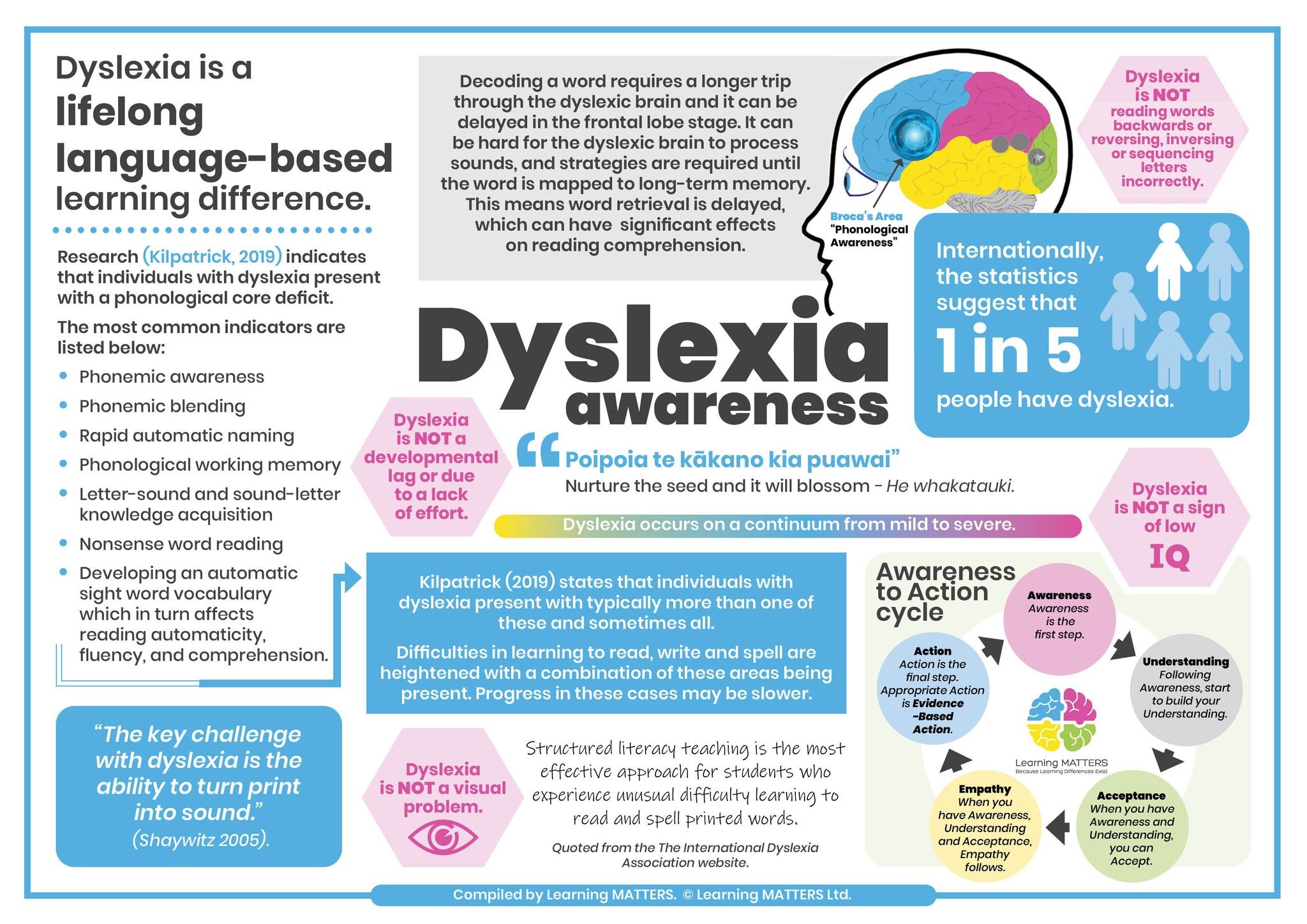
Dyslexia
Dyslexia is a common learning difficulty that is neurologically based. It affects roughly 1 in 5 people.
Symptoms of dyslexia may include reading and spelling difficulties caused by:
Difficulty with fluent word recognition
Trouble encoding and decoding words
Inability to recognize rhyming patterns
Difficulty learning the names of alphabet letters
Difficulty associating letters with their sounds.
Secondary consequences of dyslexia may include problems with reading comprehension and reduced reading enjoyment. Having decreased reading experiences can then lead to reduced vocabulary exposure.
Certain types of reading instruction are more effective for people with Dyslexia, such as Orton-Gillingham and other multisensory approaches to literacy. Paired visual and auditory information, simplified directions, examples of correctly completed work, outlines and graphic organizers, and extended time for completing assignments/tests are examples of a few accommodations that may benefit learners who are diagnosed with dyslexia in academic settings.
Source: https://dyslexiaida.org
Down Syndrome
Down Syndrome occurs when an individual has a full or partial extra copy of chromosome 21. This additional genetic material can affect a person’s body in a variety of ways including physical characteristics, medical issues, and developmental concerns.
Physical Characteristics:
Small stature
Upward slant of the eyes
Smaller nose with a flattened nasal bridge
A narrow, shortened hard palate
Short neck
Smaller head
Excessive flexibility
Low muscle tone
Medical Issues:
Heart defects
GI issues
Seizure disorders (particularly later in life)
Higher rates of infection
Musculoskeletal issues
Vision and hearing concerns
Developmental Concerns:
Cognitive delay
Feeding (ability to manage food, selective eating, etc.)
Speech sound errors/poor speech intelligibility (often due to low muscle tone; characterized by imprecise articulation, fluency type errors, vowel errors, reduction of consonant cluster, final consonant deletion, inconsistent errors, and overall reduced speech intelligibility)
Expressive and receptive language disorders
Airway concerns (increased open mouth posture/mouth breathing, sleep quality issues)
Treatment for individuals with Down Syndrome typically include speech therapy, occupational therapy, physical therapy, special education services, and of course any medical intervention needed. Just as with most conditions, people with Down Syndrome are affected on a spectrum. Some individuals have more involved symptoms, while others show milder symptoms.
Source: https://www.verywellhealth.com/symptoms-of-down-syndrome-1120463
Sensory Processing Disorder
Sensory Processing Disorder (SPD) occurs when a person has difficulty managing sensory input. Different sensory systems can be affected in a variety of ways, making SPD look different in each individual. We have 5 external sensory systems (sight, smell, taste, hearing, and touch) and 3 internal sensory systems (vestibular, proprioception, and interoception).
Typically, those with sensory processing difficulties are one of the following:
Under-responsive (meaning they are less sensitive to stimuli and require more input to elicit a response)
Example: Craves movement, enjoys bright lights or loud noises, demonstrates “risky” behavior to increase sensory input
Over-responsive (meaning they are highly sensitive to stimuli and require much less input to elicit a response)
Example: Particular about the fabric they wear, doesn’t like certain food textures, covers ears around loud noises
Have a mixed sensory profile (under-responsive in certain sensory systems but over-responsive in their other sensory systems)
Example: May crave sensory input activities like swinging, jumping, lighted/spinning toys (vestibular and visual sensory systems), but also like only certain food textures (taste/touch), or may become overstimulated easily by environmental noises (auditory).
Some people are also sensory-seekers (typically under-responders) while other people may be sensory-avoiders (typically over-responders). This factor can be impacted by whether the person actively tries to manage sensory input, or whether they allow sensory experiences to happen to them passively. Everyone has sensory preferences and falls somewhere on the continuum between too much responsiveness and too little responsiveness; however, people without SPD are able to process the input without experiencing distress and they may regulate themselves or make environmental changes to return to a regulated state more easily.
Augmentative Alternative Communication (AAC)
Augmentative and Alternative Communication (AAC) is not a disorder, but rather a term that describes various communication methods that some individuals with disabilities rely on to effectively communicate.
These methods can be:
An alternative to verbal communication (usually when a child/adult is unable to functionally communicate using verbal language), or
Can augment (support) verbal communication as needed (people with poor speech intelligibility, difficulty communicating verbally some days but be able to communicate verbally with more ease at other times).
AAC may include high-tech devices like a speech generation device with an extensive vocabulary, low-tech supports like a one-page communication board, using manual signs like American Sign Language (ASL), and everything in between. There is also a wide variety of access methods, which is of great benefit to individuals with physical disabilities or those who can’t access “traditional” devices. For example, switches can be placed near a hand or the head to allow the user to scan through the system when they’re unable to use fine motor skills to select desired words.
AAC can enable people with complex communication needs to express themselves, exercise choices, and have a sense of autonomy in their daily activities that may not otherwise be possible. Some AAC users may actually be verbal, but prefer to use AAC strategies when verbal communication is especially difficult. For example, children and adults with Childhood Apraxia of Speech (CAS) demonstrate varying levels of control over their tongue, lips, and jaw to produce speech the way they want. On “good” communication days, they may communicate verbally with little to no difficulty. However, on difficult communication days, they may prefer some kind of AAC as a less effortful/exhausting form of communication.
We hope this information was helpful! Did you learn something new? Do you have questions? Comment below!
Resources and References:
https://sensorycoach.org/the-eight-sensory-systems/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7214749/
https://www.adhdawarenessmonth.org/
https://sensoryhealth.org/basic/sensory-awareness-month-2020
https://www.mayoclinic.org/diseases-conditions/down-syndrome/symptoms-causes/syc-20355977
https://www.verywellmind.com/adhd-in-girls-symptoms-of-adhd-in-girls-20547
Bunton, K., & Leddy, M. (2011). An evaluation of articulatory working space area in vowel production of adults with Down syndrome. Clinical Linguistics & Phonetics, 25, 321-334.
Kent, R. D., & Vorperian, H. K. (2013). Speech impairment in Down syndrome: A review. Journal of Speech, Language, and Hearing Research, 56(1), 178-210.